Mandesh Institute of Pharmaceutical Science and Research Center, MhaswadDepartment of Pharmaceutics, The Oxford College of Pharmacy under Rajiv Gandhi university of health sciences, 6/9 beguru main road, Hongasandra, Bengaluru-560068
Migraine is a neurological disorder which mainly affects the neurons in the brain from degranulation of peptides which further leads to release of certain histaminic hormones that causes severe pain and chronic headache along this, the patients also feel nausea and vomiting with the migraine attack. Hence this migraine headache should be treated quickly. The conventional dosage form has very low bioavailability since it goes through GI tract by having first-pass metabolism. In the above case ODT formulations promise a rapid and effective in delivery of the drug and treating migraine attacks. Still these tablets are having problem with respect to the taste of drug. Among the drugs to treat the disorders of brain like schizophrenia and migraine, taste of most drugs are bitter. This bitter taste should be masked while formulating the ODTs. This makes challenging for formulation of ODTs. By delivering the dosage form with masking the bitterness the patient compliances increases. The ODTs are having very quick disintegration due to the Superdisintegrants and this fast disintegration is followed by the dissolution. So, the drug molecule undergo absorption within the stomach and intestinal part of GI tract by showing unavailability in the further parts like liver in which, the most of the drugs will be degraded by metabolism. Hence the ODT formulations help in treating the migraine attacks within a short period of time and with the great patient compliances.
Migraine is a neurological disorder that is concerned with severe episodic headaches, casually on either one side of the head. This affects greater than a billion individuals across the world and it is a common disorder of neurological conditions. It’s most common in the young adults and even in the females. This is associated with a vast range from stress and sleep disturbance till suicide. Instead of being common, it is so poorly detectable and it’s often undertreated. Only those neurologists, who have the knowledge to provide care for this, because it can occur from the interaction between genetic and environmental factors. Some investigations on monogenic migraines had resulted in strong link between migraine and neurovascular disorders and they also reported that more than 180 variants found in the vascular and neuronal tissues that very variant enriches the risk of migraine, those are predisposing for migraine. These also results in causing nausea, vomiting, and some sensitivity to movement, sound and light that the person with the migraine will feel difficulty to sustain any type of sound and light and also, they will restrict their movements. According to ICHD-3 (International classification of headache disorders- 3rd version) the prodromal phase has preceded till 48h with the symptoms like mood changes, photophobia, fatigue, neck pain, yawning, dizziness, craving and difficulty in concentration. Some elements can trigger this migraine such as stress, odors, foods and alcohol. And the above elements are categorized on the bases of their occurrence such as endogenous triggers and exogenous triggers. The postdrome phase of migraine includes fatigue, neck stiffness, increased appetite and dull head pain. [1] Studies have reported several risk factors for the attack of this migraine. The survey disclosed that insomnia, depression, anxiety, gastric ulcers, angina and epilepsy were high among migraine patients. And the pain in the migraineurs is dependent on both psychological and biological disorders also due to inflammation. It also affects the hormonal levels; due to this imbalance in the hormones will influence pain-processing networks in the brain. Some of those hormones affecting migraine are Estrogen, cortisol and thyroid hormones. Since the estrogen hormonal imbalance is a cause for this migraine. The females suffer at double the rate of men from the pain of migraine. Menstrual migraine is a condition where the sudden drop of estrogen levels at a few days before menstruation. However, based on current information on migraine. It shows a vast range of triggers and risk factors. These can be managed in certain ways to reduce the rate of recurrence and severity of pain in a migraineur by informing them regarding the causes and the risk factors. Also, some aerobic exercises can manage the duration of migraine attacks and by the administration of estrogen for premenstrual and menopausal women can reduce the effectiveness of migraine headaches.[2] Patients think headaches as migraine but The International Headache Society in the book of International Classification of Headache Disorders (ICHD-II) they made different headache terminologies that according to their sever pain that have been experienced by the several patients over the centuries. There are different types of migraine according to their occurrence and their severity. They are classified as the follows:
Where Migraine without an aura was earlier named as “common migraine” and Migraine with an aura was known as “classic migraine”. Among these two most of the people got effect by common migraine, only 18% of people affected by classic migraine. Also, over 13% of people were affected by a combination of migraine with and without aura. Other migraines like Childhood periodic syndromes are commonly precursors of migraine concerns with pediatric conditions while Retinal migraines cause monocular visual disturbance preceding migraine headaches. The Complications of migraine associated with ischemic infraction of brain or to epilepsy and the probable migraine do not meet diagnostic criteria. [3] Above information on migraine shows its effect for the society and the pain for the patient. So, it needs to be treated quickly to reduce the pain caused by it. The conventional dosage forms those are formulated as tablets have some issues of bioavailability and potency. So, to get good bioavailability we need to formulate the tablets that skip the first pass metabolism. Since the conventional dosage form for migraine has the metabolism property in the liver. The drug should be absorbed within the stomach and small intestine so it will not get metabolized in the liver. To formulate the dosage forms as such, we have to consider either by formulating in the liquid form or in the form of ODTs (Orally disintegrating tablets). The liquid formulation will be having issues with the stability. So, the ODTs will be best for the treatment of migraine. To overcome these medical needs, the pharmaceutical technologists have formulated advanced oral dosage form known to be Orally Disintegrating Tablets. These tablets readily disintegrate with the help of saliva in the mouth, normally in a matter of less than a minute, regardless of taking water. So, the dissolution and absorption of the drug will be in the stomach and small intestine. So, onset of clinical effectiveness and drug bioavailability of the dosage form may be significantly higher than the conventional dosage forms. Though chewable tablets are there in the market, they make difficulty for the patients, who feels painful to chewing and for the children those lost their primary teeth. In these conditions the ODTs plays a very important role in easy providing the best dose for the patients. The recent studies given magnificent preference for the ODTs by many patients and more consumers would recommend their doctors to prescribe ODTs to regular tablets pr liquid.[4] ODT formulations have been formulated for maximum indications, those ranging from migraine (which needs immediate onset of action) to mental illness (in which patient compliance plays important in treatment of depression and schizophrenia) due to their promising delivery in treating those disorders which causing the heavy episodes of pain in the patients.

ODTs are alike from conventional dosage forms such as sublingual, buccal and lozenges, which needs more time to dissolve in oral cavity. They also have synonym of Oro-disperse, mouth-dissolving, quick-dissolve, fast-melt and freeze-dried wafers. The main advantage of this ODTs are, they do not need water and chewing before swallowing and these are produced to dissolve within few seconds those are known as true oral disintegrating tablets. They use some agents which help them to increase their disintegration in our oral cavity and the agents are known as super-disintegrants. The aim of these new orally disintegrating tablets dosage formulations are generally been for geriatric, pediatric, bedridden and some developmentally disabled patients who suffers from persistent nausea while travelling or in case of water unavailability. The main advantage of these ODTs is that it will merge the advantages of both liquid and conventional formulations. These drugs start getting absorbed from mouth, pharynx and esophagus as it passes into the GIT; in this case it helps in increasing the bioavailability of the dosage forms by making the drug readily available to absorb at my point of Gastro-intestinal tract and it will decrease the first-pass metabolism by making the drug to absorbed before reaching the part in which the drug has the degradation property by metabolism. Also, it makes easy for the unwilling patients in administration. [5]
The presently available ODTs have the combined and advanced formulations which include improving taste masking, making modified release of the dose and enhancing or advancing the bio-availability of these ODTs. As a result, in the present scenario the formulator can mask the taste of even the drugs that have extremely poor-taste. Some new ODTs contain rapidly dispersing micro granules formulated by direct compression with lubrication on external tablets. These stated excellence in physical robustness, feel in mouth and disintegrating phenomenon of the tablet. These tablets dissolve within 15-30 seconds and produce smooth and pleasant taste of API and excipients mixture. This is done by combining micro-encapsulation with ODT technology. One such technology is based on coacervation, that place a uniform coating of polymer membranes on the dry crystals of ODTs directly and forms particles of size 150-300 microns. This forms an inert barrier between the API and taste buds and also stable barrier between API and excipients and results in greater taste masking property for the ODTs. The formulation of controlled release combining with ODTs by some special polymers and coating processes those produce the ODTs with sustained, modified and customized dose release profiles in ODTs. Also, the combination of release profiles within a single dose also possible in formulations. All of these are following the approaches by micro-encapsulation and multi-particulate coating which makes the modified release polymers on the API. These polymers give the physical strength for the ODTs also helps in gives good mouth feel for the patients and results in good patient compliances. The absorption takes place immediately after the release by making this dose to enter the systemic circulation. Since the disintegration and the dissolution will be taking place within a small period of time, the drug attains the specific therapeutic level and so evokes pharmacological action of the dosage form. Due to the starting of disintegration in the early part of GIT; some factors like GI pH, blood flow throughout the GIT is studied to take advantage of the microenvironment of the GIT to increase the absorption or bioavailability of the dosage forms. In the geriatric patients, decrease in their body mass, total water content in the body will imply with decrease in volume of distribution for the water-soluble drugs and also increases volume of distribution for the lipid soluble drugs. Also, the liver volume decreases and the blood flow to the liver also get reduced. Hence, the metabolism of the drug in the liver from the oxidation, reduction and hydrolysis also decreases. Thereby the renal clearance of drugs gets slowed. So, the half-life of the drug also increases. [6]
The APIs used in the ODT preparation have majorly act systematically i.e. it will get into systemic circulation to give the desired therapeutic activity instead of local effects. These drug properties should not alter the considerable tablet properties. Few of the characteristics such as solubility, morphology, size of particles, moisture holding capacity and compressibility of the APIs will affect the ODT features in the final. Thus, there are few criteria for an API to be used in the preparation of ODTs that makes the qualitative, effective and acceptable tablets. Those criteria are as follows:
The excipients in ODTs also play an important role in formulation of effective and qualitative product. These excipients when blended or formulated with the API, they should not react with one another. The occurrence of any internal degradation by the effect of excipients may occur. So, the considerations of certain requirements to be fulfilled are as follows:
The excipients used for the preparation of ODTs are Super disintegrants; which are used to decrease the time of disintegration, Bulking materials; also known as diluents and use for increase the bulk volume of preparations, sweeteners; those helps in masking the taste of the formulations and Flavor; which helps in altering the unpleasant odor of the formulations. These sweeteners and flavors are added for giving the good patient compliance to adhere to the dosage form.
Table 1: Excipients used for the formulation of ODTs. [8]
|
Excipients |
Function |
Examples |
|
Superdisintegrants |
Enhance the disintegration of the tablet, thereby increases the dissolution and the absorption of the drug increases. So, it helps in the enhancement of bioavailability. |
Crospovidone, sodium carboxy methyl cellulose, Carboxy methyl cellulose, Microcrystalline cellulose, etc. |
|
Binder |
Binds the content in a dosage form and holds it in a tablet form prior to the administration. |
Polyvinylpyrrolidone, Polyvinyl alcohol, Hydroxy propyl methylcellulose, etc. |
|
Fillers |
Increases the Bulk of the tablets. |
Mannitol, Lactose, Sorbitol, xylitol, calcium carbonate, magnesium carbonate, calcium phosphate, calcium sulfate, etc. |
|
Surface Active agents |
It decreases the interfacial tension in between the particles in the dosage forms. So, enhances the solubility. |
Sodium doecyl sulfate, sodium lauryl sulfate, Tweens, Spans, polyoxyethylene stearates, etc. |
|
Lubricants |
This reduces the friction between mechanical moving parts of machines used in formulations. |
Stearic acid, Magnesium stearates, Zinc, calcium state, talc, polyethylene glycol, liquid paraffin, magnesium lauryl sulfate, etc. |
|
Sweeteners |
Sugar based bulking agents exhibits impart sweetness taste for the formulation. |
Aspartame, dextrose, fructose, isomalt, lactilol, maltitol, maltose, mannitol, etc. |
|
Color |
Brighten the appearance of the dosage form as enhancement of organoleptic properties. |
Sunset yellow, Amaranth, Red iron oxide, etc. |
|
Flavors |
Increases Patient compliance and acceptability |
Peppermint flavor, clove oil, bay oil, anise oil, eucalyptus oil thyme oil, vanilla, citrus oils, fruit essences, etc. |
In the year 2014 M. K. LADOLA, et.al., investigated on multifunctional co-processed Superdisintegrants such as Crospovidone and Kyron T-314 by preparing melt-in-mouth tablets with the help of solvent evaporation method and they done different evaluation test for the formulations such as hardness, friability, in-vitro disintegration, in-vitro dissolution time, wetting time, ratio of water absorption and drug content. The results of their study gave the excellent flow property, high compressibility, reducing disintegrating time to 5.70 second and dissolution time of 9.71 seconds of the 10th formulation with co-processed Superdisintegrants in the ratio of 1:1 among all formulations.[9] Recently in 2024 the Dongyue Yu, et.al., had worked on the impact of diluents on the compaction, dissolution and physical stability of amorphous solid dispersion tablets and they have started with the four normally used diluents such that microcrystalline cellulose (MCC), anhydrous lactose, starch, and mannitol are selected for the study. They come up with the results of the ASD tablets which are prepared using MCC have highest mechanical strength compared to other diluents, ASD tablets which have lactose and mannitol had given the faster release rate than the others. Overall, the study had given the importance of choosing the excipients; considering the mechanical strength and the rate of release of the tablets, leading to improved manufacturing with qualitative and effective dosage formulations. [10]
The phenomenon of preparation of a dosage form by the combination of all required APIs and excipients in particular ratio in formulation of qualitative and effective dosage form. This formulation contains different technologies in the ODTs preparation that are:
5.1 Direct compression: This process includes the use of conventional equipment’s with common excipients. This is one of cost-effective technique with the limited steps in processing such the using the available excipients with certain quantitative ratio with the API and homogeneously blended. Then the blended mixture is compressed with particular pressure in the compression machine.
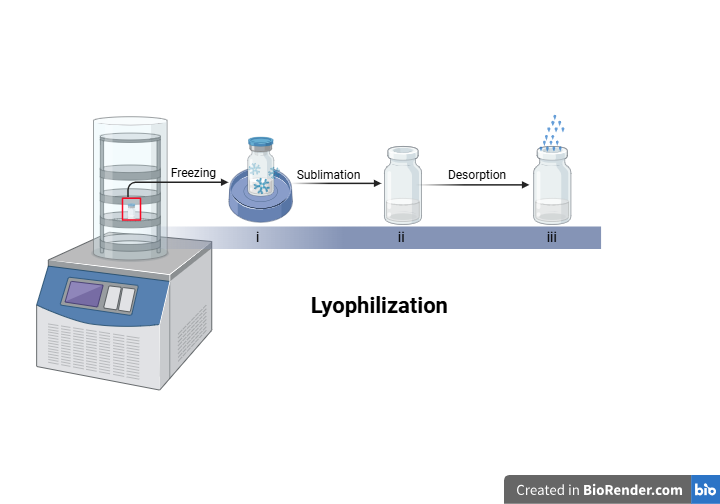
5.2 Lyophilization or Freeze-Drying: This process consists of the removal of solvents from the drug solution which was in the frozen form or from the suspension that contain the structure-forming excipients. There are three different phases of this process:
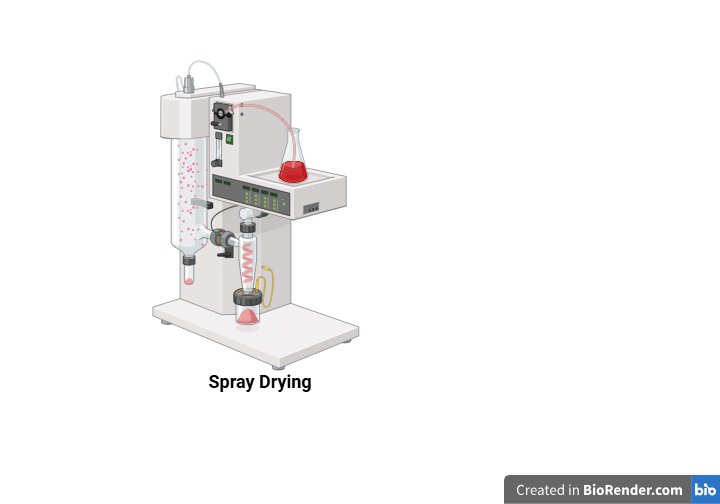
5.3 Spray drying: In this process the aqueous part of the materials containing the matrix and other ingredients are dried with the help of spray drying then the API is added and make a tablet by compression. The tablets made by following spray drying have a disintegrating time within 20 seconds. This is due to the formation of extremely porous and fine powder on drying the ingredients.
5.4 Molding: In this the blend of all ingredients are pushed through a tiny pored screen and they are mixed through hydro-alcoholic solvent for moistening the content then molded as a tablet. These molded tablets have disintegrating time more rapidly and also mask the taste.
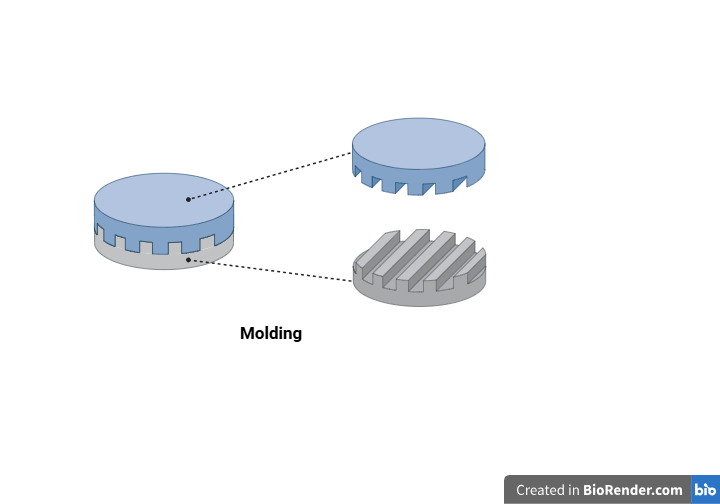
There are different molding techniques to prepare ODTs follows:
5.4.1. Compression molding: This is the normal phenomenon of compressing the moistened powder blend with hydro-alcoholic solvent followed by drying to remove the solvent.
5.4.2. Heat molding: The solution or suspension of the drug, agar and sugar are formed and they are filled in the blister packs. They are then solidified to form jelly structure at room temperature, then dried at 30°C under vacuum to form the tablets.
5.4.3. Molding by vacuum evaporation without lyophilization: this process follows the evaporation of the solvent from the solution of drug. This uses the pressure to evaporation of free solvent from solid through the liquid part of the gas.
5.5 Phase transition process: In this, the compression of two sugar alcohols which are having higher or lower melting point then they are going to heat it at 93°C for 15 min. this increases pore size and the hardness. Kuno et,al., have worked on the effect of preparation method on the properties of orally disintegrating tablets manufactured using phase transition of sugar alcohol. They have resulted that the hardness of tablets increased to 6kp due to the heating process but the disintegrating time of the tablet that have the talc has not changed even though the increase in the hardness. So, they have mentioned that the polarity of the tablets containing talc had increased its harness after heating. This indicated that the more hydrophilic surface can be obtained on heating the talc. [12]
5.6 Melt granulation: In this the pharmaceutical powders were clustered by the use of binder. The powder was heated to above melting point of the binder that helps in forming the solid dosage form. This heating is done by the heating jackets or by the friction force that formed from the impeller blades. The abdelbary, et.al., were worked on the preparation of orally disintegrating tablets using a hydrophilic waxy binder. Here they have used PEG 6-stearate which has the melting point of 33-37°C with the HLB value of 9. This binder with the other ingredients were heated above the melting point of PEG 6-stearate to prepare molten mixture of drug and the excipients before formulation the final dosage form. So, with the binding property it also increased the physical resistance of the tablets and also it helps in disintegration of the formulation due to their melting phenomenon in the moth. [13]
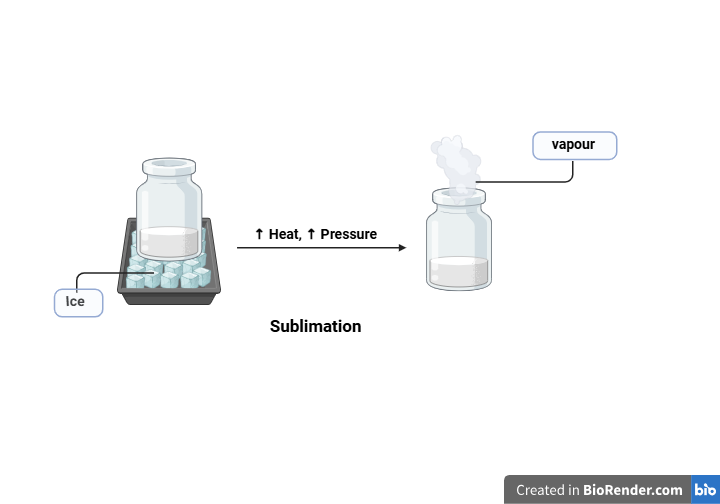
5.7 Sublimation: In this all the ingredients were mixed with the volatile ingredients like camphor, ammonium bicarbonate, urea, etc. then the entrapped volatile ingredient is taken off by the sublimation method. That formulates porous powder. Then the powder will be compressed to formulate the tablets.
5.8 Oral Disintegrating Thin Films: In this the hydrophilic film forming polymer with the drug and the other taste masking agents were dissolved in the non-aqueous solvent. This will produce the non-aqueous solution; this will lead to formation of thin film after the evaporation solvent.
The attack of migraine can be divided into phases in related to the headache. This is classified on their time period and the extent of the pain for the patient. These phases will help us to distinguish the pathophysiological changes that are taking place in the patients. They are as follows:
In the premonitory phase, there are several symptoms that include; polyuria, irritability, mood change, yawning, neck pain, concentration difficulties and light sensitivity. These are commonly occurring just an hours before the onset of migraine attack. In this condition the PET and the functional MRI studies of patient will give the changes occurring in the activity and connectivity of the hypothalamus and increased activity of occipital cortex. This may take to some of the symptoms like polyuria, mood change, small change in appetite and light sensitivity by occipital cortex exaggeration. In this phase it also affects a mediator, cutaneous allodynia in the thalamus. These changes in the thalamic and thalamo-cortical activity will form a key part to the central feature of migraine attack and act as a therapeutic target for the prevention of migraine. Some studies like resting state MRI scan will show the altered connectivity to thalamus, hypothalamus, brainstem, amygdale and cerebellum which are responsible for changes in the multiple overlapping sensory nerves and modulate the pain caused by the migraine attacks. The aura phase includes the increased risk of some comorbidities such as perioperative stroke, Parkinson’s disease, restless legs syndrome, panic disorder and bipolar disorder. This occurrence of aura phase in the migraine attack and clinical features and even the location of the starting of aura within visual field are variable between the patients. During some times the progressing aura phase will not give any significant change in visual activity. So, migraine aura commonly occurs without headaches and more of the migraines even won’t include the aura. This concludes that the aura is not necessary for the headache. The headache phase is the phase where the patient will feel much pain starting from a place in the brain and it will propagate throughout a side of brain. Followed by the postdrome phase, that includes some depolarization and dysfunction of the brain nerves and cells causing the pain of migraine attack.
CGRP: This calcitonin gene-related peptide will be released into the circulation during the migraine. This CGRP concentration normalizes only with the triptan therapy and some small molecule CGRP antagonists as acute migraine therapies. But a study made with the peptide release of some patient shown the no increase in the concentration of vasoactive intestinal peptide, substance P, and Neuropeptide Y. So, the CGRP release will not define the generalized neurogenetic inflammation. The efficacy of antibodies that are targets the CGRP or its receptor plays a vital role in understanding of Pathophysiology of migraine. This CGRP cannot cross the BBB in considerable concentration. So, targeting this CGRP outside the brain may prevent migraine.
PACAP: The pituitary adenylates cyclase-activating polypeptide also acts as a mediator for the migraine parallel to the CGRP. The triggering of migraine when systemic administration of this PACAP for certain individuals and also the elevated concentration of PACAP is reported in the patients of migraine. Therefore, PACAP represents an encouraging therapeutic target for the migraine. The PACAP has two forms of bioactive element such as having a 38-amino acid peptide (PACAP38), and having a 27-amino acid peptide (PACAP27). Among these the PACAP38 acts as a neurotransmitter, a hormone and a neuromodulator. The PACAP38 causes the degranulation which further responsible for the release of histamine which causes the inflammatory response, and this response mainly effects through VPAC1, VPAC2 and PAC1 receptors. Out-off these the vasodilatation and mast-cell degranulation are arbitrated from VPAC1-2 receptors and PAC1 receptor will associated with multiple physiological function which also includes chronic pain of the migraine in which the patient experiences the pain in one side of brain which actually caused by these mechanisms so by targeting this PACAP might be helpful for the treatment of chronic migraine headache. [15]
TREATMENT: [16]
The vasodilatation may be a cause for the migraine pain and it seems to be intracranial and extracranial vasodilatation in cluster headache but the vasoconstriction might not be preferred for the abortion of both the migraine attack and cluster headache. So, the triptans such as serotonin 5-hydroxytryptamine receptor agonists are known to be abortive therapy in migraine also for cluster headache with the oxygen therapy by having grater neural based actions. Also, the ergotamine is used to manage both the disorders. This biology has made the scope of therapeutic treatment targets for the migraine and cluster headache. The series of randomized trials of some 5-HT1F receptor agonist, for the treatment of acute migraine have an efficacy even in case of difficulty to treat attacks also in triptan non-responders. These also identified some dizziness as an adverse effect of these treatments. So, by trying a novel approach it won’t cause vasoconstriction and therefore they give the safest treatment for the migraine and even for the population having the cardiovascular disorders. By understanding several facts of migraine, targeting vasoactive Neuropeptides had become considerable area of interest for the treating migraine and cluster headache therapeutics.
These Orally disintegrating tablets are very useful replace for conventional oral dosage forms which have the problems of difficulty in swallowing and the patients who feel nausea and vomiting while swallowing tablets, these conditions may affect the absorption of the dosage forms. So, this is the important subject to consider because epidemiology of the migraine reveals that majority of migraine patients have been experienced nausea during their migraine attack. Thus, the novel formulations like orally disintegrating tablets give opportunity for the patients to use these dosage forms without a need for liquids and also, they may be taken on site of migraine attack. These are formulated with the aim of offering convenience and tolerability to the patients in taking the tablets as a treatment. There are currently only two oral disintegrating tablets for migraine, they are rizatriptan and zolmitriptan. Among this the rizatriptan oral disintegrating tablets are having high effects in clinical and in their pharmacokinetic profile but the preclinical studies of zolmitriptan ODTs are having similar to the conventional tablets. [17] In the year 2020, the author Alicia potter DeFalco, et.al., Were worked on the Rimegepant orally disintegrating tablet for acute migraine treatment: A review. They were studied the pharmacology, pharmacokinetics of Rimegepant ODTs and observer that they have limited adverse effects, rapid onsite of action and duration of relief from the ODTs. This made them as promising treatment for acute migraine headaches. [18] In the year 2012, Jeffrey L. Seeburger, et.al., were made a research on Rizatriptan for Treatment of Acute Migraine in those Patients Taking Topiramate for the Migraine Prophylaxis and they observed that, about two hours there been significantly higher pain relief with rizatriptan compared to placebo. It also showed the constant pain relief about 2 to 24hours. So, they concluded that these ODTs were superior at the pain relief and in the treatment of acute migraine headache. Suggested that, using Topiramate will not affect the effectiveness of rizatriptan in the treatment to acute migraine. [19] In the year 2010, Ravi s heshala, et.al., were worked on Formulation and Optimization of Orally Disintegrating Tablets of Sumatriptan Succinate. In this they prepared microspheres by coating Eudragit over sumatriptan succinate. Then they formulated ODTs using different concentration of Superdisintegrants out of 31 formulations they found that F28 was optimized formulation with the disintegration time of 41seconds. And all other formulations were found within the limits of pharmacopeia. And concluded that, microspheres with a ratio of 1:1 were masked the bitter taste of sumatriptan. Hence, this ODT as a “patient-friendly dosage form” is useful alternative to available conventional tablets. [20] In the year 2002, AJ Dowson, et.al., were studied on Zolmitriptan orally disintegrating tablet is effective in the acute treatment of migraine. In this about 471 patients were provided with the zolmitriptan oral disintegrating tablets of 2.5mg to treat severe migraine. They reported that the formulations are effective for about 1-4 hours pain-free response for the migraine attack. Among the patients who received these ODTs, 70% of patients prefer zolmitriptan oral disintegrating tablets over the conventional dosage forms. [21]
CONCLUSION:
The oral disintegrating tablets are the preparation those disintegrate themselves when they come in contact with saliva in our oral cavity so the disintegration of the tablet will start from the oral cavity itself. This will make the drug to be in liquid form in the early stages of gastrointestinal tract. So, the drug will be readily absorbed within the stomach and intestinal area in the gastrointestinal tract hence, the drug will not get exposed to the enzymes in the liver. So, the loss of the dose also decreases and it leads to enhancement of bioavailability. Since it gives high bioavailability within a short period of time the drugs which are used to treat some emergency disorders or some diseases those causing the severe distress may formulated by this method to treat the condition. The migraine is one of such diseases in which patients feel the headache with severe episodes. It had said that this pain is caused by some Neuropeptides like CGRP and CAPAC, these will degenerate and release the histamine like hormones by mast cell degranulation, which redirect to vasodilatation and leads to multiple physiological conditions like migraine attacks including chronic pains. Hence the drugs that used for treatment of migraine have to be rapid in their onset of action. Since the patient needs an accurate amount of dose in attributed time, the conventional dosage forms will take time for onset of action also with the loss of some amount of drug in the name of first-pass metabolism. So, the formulation made with ODTs will give rapid onset of action with high bioavailability will be greater valued innovations for delivering the treatments. The drugs of bitter taste will form inconvenience for the patients but that bitterness can be modified or masked in the formulation of oral disintegrating tablets. By this the ODT formulations have made best-fit for the treatment of migraine like disorders.
REFERENCES


Rakesh A. M.*, Gururaj S. Kulkarni, Anna Balaji, ODTs (Orally Disintegrating Tablets): An Improved Rapid Treatment to Migraine, Int. J. Med. Pharm. Sci., 2025, 1 (11), 56-67. https://doi.org/10.5281/zenodo.17566127
 10.5281/zenodo.17566127
10.5281/zenodo.17566127
