Clinical Trial Assistance at Lambda Therapeutic Research
Migraine is a prevalent disabling illness in the adult population, with a female predominance. Unilateral throbbing headaches of moderate to severe severity are a typical migraine manifestation, however they can present in a variety of ways. Despite significant advances in pathophysiology understanding, which has led to the development of innovative treatments, evidence-based migraine treatment remains an unmet need, particularly in underdeveloped nations. This article discusses the pathophysiology, diagnosis, and evidence-based approach to migraine treatment.
Recurrent headaches are one of the most frequent nervous system illnesses. Headache is a severe and disabling symptom of a few major headache diseases, including migraine, tension-type headache, and cluster headache. [1] Among these, migraine headache is widespread, common, disabling, and essentially treatable, although it is nevertheless underestimated and undertreated. [2] Migraine is a common chronic headache illness characterised by recurring attacks lasting 4-72 hours, pulsing in nature, moderate or severe in intensity, exacerbated by normal physical activity, and accompanied by nausea, vomiting, photophobia, or phonophobia. [3] It is referred to as the seventh disabler due to its significant impact on the patient's quality of life (QOL). [4] It is the most common cause of headaches in youngsters.
PATHOPHYSIOLOGY
1. Vascular and Neurogenic Theories Migraine headaches are still not fully understood. Historically, two independent ideas have been offered to explain the origin of migraine headache: the vascular theory and the neural theory. Thomas Willis proposed the vascular theory, stating that "all pain is an activity violated" and arguing that headache pain is generated by vasodilation of the cerebral and meningeal arteries. The alternative neurogenic theory focuses on the source of migraine pain, which is now associated with trigeminovascular system activation. [6]
2. Cortical Spreading Depression The alternate and commonly accepted explanation holds that the aura is caused by cortical spreading depression (CSD), which is a wave of neuronal hyperactivity followed by an area of cortical depression, and that the headache is caused by trigeminovascular pain pathway activation. Atypical pain processing, central and peripheral sensitization, cortical hyper excitability, and neurogenic inflammation all contribute to Chronic Migraine (CM). Cortical hyperexcitability is regarded to be another important element in the transition of EM to CM. [4]
3. The exact cause of migraine attacks, as with many other episodic diseases, has yet to be determined. Many clinical factors, including food, sleep changes, and stress, are known to predispose people to attacks. It's especially noteworthy that photic stimulation can cause both migraine headaches and epileptic convulsions. It's unclear how these things trigger a migraine attack. However, there is evidence that migraineurs have greater cortical response to a variety of stimuli. The approaches that have been utilised to create this data include psychophysical studies; visual, auditory, and somato ceptive evoked potentials; magneto encephalography; and transcranial magnetic stimulation of the motor cortex. All instances show signs of increased responsiveness between migraine bouts. The findings from transcranial magnetic stimulation of the occipital (visual) cortex have been particularly striking. Most, but not all, studies have found that migraineurs have a lower threshold for inducing phosphenes (the perception of light with non-luminous stimulation) than controls. This phenomenon appears to occur equally in people who get migraines with and without an aura. Thus, migraine may be defined by a pathologically low threshold for cortical hyper excitability activation. [7]
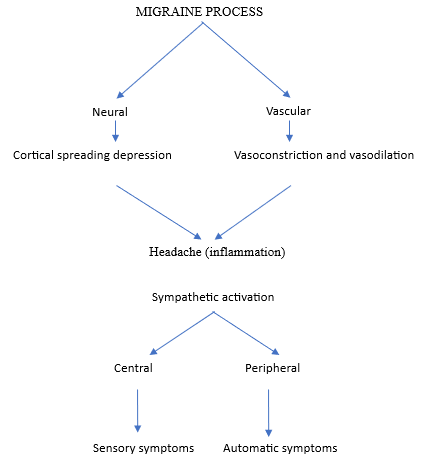
Fig. 01 Pathology of Migraine
Trigger for Migraine
Mollaoglu M conducted a study and found that the most common trigger variables were emotional stress (79 percent), sleep disturbance (64 percent), and dietary issues (44 percent). [8] Sleep and stress were significant triggers in migraine with aura patients, whereas environmental factors were strong triggers in migraine without aura patients. Stress, sleep, and environmental factors were significant triggers for women compared to men. Trigger factors are common in migraine patients, and avoiding them may lead to improved condition control. [8]
CLINICAL FEATURES
Women had an 18% risk of migraines, compared to 6% for men. The higher occurrence in women is usually related to hormonal swings, namely oestrogen. Migraines often start at adolescence or between the ages of 35 and 45. [9] Migraine includes two basic subtypes: migraine with aura, which is distinguished by transitory focal neurological symptoms that frequently precede or accompany the headache. Some patients have both a premonitory phase, which occurs hours or days before the headache, and a headache resolution period. Hyperactivity, hypoactivity, and depression, as well as cravings for specific foods, recurrent yawning, weariness, and neck stiffness or discomfort, are examples of premonitory and resolution symptoms. Migraine without aura is a clinical syndrome characterised by headaches with specific features and associated symptoms such as unilateral location, pulsating quality, moderate or severe pain intensity, aggravation by or causing avoidance of routine physical activity, nausea and/or vomiting during the headache, and photophobia and phonophobia. [10]
DIAGNOSIS
Migraine can be diagnosed by obtaining a history. Alternatives are ruled out using orthopaedic testing, cranial nerve examination, complete blood count, urine, and, if necessary, cranial magnetic resonance imaging. [9] The International Classification of Headache Disorders defines migraines using the following criteria. [10]
TREATMENT
Non-Pharmacological Treatment
Migraine is the most prevalent type of headache that prompts sufferers to see a doctor. To control the headache condition, most patients should receive a combination of non-pharmacological and pharmaceutical therapies. Many non-pharmacologic remedies are based on the theoretical premise that migraines are caused by neurochemical instability in the brain. These approaches, which are frequently referred to as "biobehavioral," may be used in conjunction with or in place of pharmaceutical treatment. William EA. et al. developed a guideline for the non-pharmacologic management of migraine in clinical practise, which includes applying cold or pressure to the head, reducing activity and sensory input in a quiet or dark environment, and attempting to sleep, and is supplemented by the use of pharmacologic therapies when insufficient in isolation. Relaxation treatment, hypnosis, transcutaneous electrical stimulation, acupuncture, and occipital or supraorbital nerve blocking have all been utilised in the acute setting and are being considered. Additional therapeutic options include biofeedback, relaxation therapy, cognitive-behavioral therapy, psychotherapy, hypnosis, and physical measures including chiropractic, osteopathy, and physiotherapy. [11] Brette R. provided a case report. et al. recommended dietary and lifestyle adjustments for migraine management. [9]
PHARMACOLOGICAL TREATMENT
Abortive treatment for migraine. The basics of abortive therapy for migraine headaches are to use analgesics sparingly, taking into account the patient's profile, headache intensity, and agent adverse effects, in order to provide immediate and lasting headache relief.
5-HT1B/1D receptor agonists:
Triptans work through 5-HT(1B/1D) receptors to cause vasoconstriction of painfully dilated cerebral blood vessels, limit the production of vasoactive neuropeptides by trigeminal nerves, and reduce nociceptive neurotransmission. [12] There are several tripans on the market, including sumatriptan, almotriptan, eletriptan, frovatriptan, naratriptan, rizatriptan, and zolmitriptan. Eletriptan, followed by rizatriptan, has a higher headache response rate and safety profile than other triptans. [13] It should not be used more than 2-3 times per week to avoid the onset of prescription overuse headaches. Individuals with cerebrovascular disease and cardiovascular disease should avoid using them.
Other analgesics:
Paracetamol, because to its low cost, widespread availability, and mild side effects, can be utilised as the first choice in migraine patients when NSAIDS are contraindicated or not tolerated. Even while paracetamol produces a better reaction than placebo, the NNT for pain response is lower than that of other analgesics. If 10 mg of metoclopromide is added to paracetamol, the effect is comparable to sumatriptan. [14] For the treatment of acute migraine attacks, 1000 mg of aspirin is equivalent to 50 or 100 mg of sumatriptan. The addition of Metaclopromide 10 mg to aspirin lowers nausea and vomiting. Aspirin causes less side effects than sumatriptan. [14] Ibuprofen 400mg in soluble form is useful at reducing the pain intensity of migraine headaches, while total relief is only achieved in a minority of cases. [15] Oral diclofenac potassium 50 mg is a successful treatment for acute migraine, providing relief from pain and accompanying symptoms, however only a minority of individuals get pain-free reactions. Adverse effects are often moderate and temporary, occurring at the same rate as with placebo. [16] Naproxen 500 mg alone is clinically ineffective for managing migraine headaches (NNT:11 for pain free response at two hours). [17] Metoclopromide 20 mg iv is equivalent to 6 mg SC sumatriptan in an emergency scenario. [18] Opioids are one option for treating the intensity of migraine headaches in an emergency context, but due to the risk of deteriorating quality of life, concomitant psychiatric co morbidities, and habituation, their usage is limited to patients for whom other first-line agents are contraindicated. [19]
Preventive therapy:
Migraine is a chronic disease that causes a patient to use abortive medication often, resulting in medication overuse headache and the progression of episodic migraine to chronic migraine. An indication for migraine prevention treatment. [20]
Flunarizine:
Migraine is a chronic disease that causes a patient to use abortive medication regularly, resulting in medication overuse headaches and the change of episodic migraine into chronic migraine. Migraine prevention treatment indication. [20]
Beta blockers:
Although beta blockers such as propranolol, atenelol, metoprolol, and bisoprolol have been demonstrated to be effective against migraine headaches, the majority of data points to propranolol as having the highest efficacy. The starting dose is 20mg/day. This must be increased gradually because unfavourable effects can appear before to preventative effects, impairing patient compliance. The prophylaxis should be continued for at least three months before efficacy is evaluated. The successful preventative treatment should last for 12 months. Then, discontinuation can be attempted, but drug doses should be reduced gradually to avoid tachycardia and hypertension. [22]
Tricyclic antidepressants:
Amitriptyline hydrochloride is the preferred tricyclic antidepressant for migraine therapy. To have the best therapeutic impact, start with 10 mg and gradually increase to 75 mg. The response to these medicines is usually within four weeks of starting treatment. Dry mouth, weight gain, postural hypotension, and drowsiness are common side effects of these medications. [20]
Divalporex Sodium:
Divalporex sodium lowers migraine attacks compared to a placebo (P-≤ 0.05). The starting dose for divalporex Sodium is 500 mg/day, which can be increased to 1500 mg/day. Its common negative effects include nausea, dizziness, and tremor. [20]
Topiramate:
Topiramate operates by inhibiting glutamatergic excitatory amino acid transmission, voltage-gated calcium channels, GABA-evoked currents, rapid Na+ channel blockage, and carbonic anhydrate inhibition. [23] It decreases migraine/migrainous headache days (topiramate -6.4 vs placebo -4.7, P=.010). Its starting dose is 25 mg/day, which is increased by 25 mg per week until it reaches a maximum of 100 mg/day. Topiramate's common adverse effects include paresthesia, weight loss, upper respiratory tract infection, and weariness. [24]
Other preventive drug:
Calcium channel blockers such as cyclendelate, nicardipine, nifedipine, and verapamil have been tested to prevent migraine headaches, but none have proven to be more effective than placebo [25]. Though ACE/ARB use is proposed for migraine headache prevention, no clinical investigation has demonstrated their efficacy in reducing migraine headache frequency by 50%.
Future direction:
CGRP receptor antagonists (CGRPRAs) are innovative non-serotoninergic migraine-specific medicines that lack a vasoconstrictor activity and are thought to be acceptable for patients with vascular illness. [26] Serotonin 5HT1F agonists like lasmiditan has proven good efficacy and tolerance as an immediate therapy of migraine headache. [27] Glutamate receptor antagonists have shown useful in the immediate treatment of migraines without aura. [28] Neuromodulation using occipital nerve stimulation (ONS) with implanted leads was investigated as a potential treatment for persistent migraine. [29] Given the documented preventive impact of sphenopalatine ganglion stimulation in cluster headache, investigations are under underway to investigate the efficacy of this approach as a potential preventive treatment for chronic migraine. [30]
Pregnancy migraine management [31-34]:
Women who suffer from migraines experience headaches soon before or shortly after menstruation. They may also change during pregnancy or menopause, then recover afterward. Some women claim that migraines develop or worsen during pregnancy. However, for many women, the attacks became more severe or did not occur until later in the pregnancy. Many women report that their headaches stabilise or even disappear during pregnancy. This could be connected to the more stable hormone levels that occur throughout pregnancy. To reduce the risk of birth abnormalities, certain migraine-prevention drugs must be discontinued before becoming pregnant. There are only a few research on drugs used to treat migraine headaches during pregnancy. Acetaminophen is relatively safe when taken at the recommended dosages. If a patient suffers from frequent headaches, his or her doctor may provide certain therapy possibilities. Many migraine drugs, including triptans, have not been extensively tested in pregnancy. Before prescribing these medications, the potential advantages to the patient must be balanced against the hazards to the foetus.
Children migraine management [35,36]:
Migraine headaches can occur in youngsters. Treatment is similar to that of migraines in adults, but drug dosages may need to be altered based on age.
Preventive medications: [37]
These medications are taken on a regular basis, sometimes even every day, to minimise the severity or frequency of migraines. Many migraine sufferers use triptans to alleviate their symptoms. Triptans operate by constricting blood arteries and inhibiting pain pathways in the brain. Triptans are excellent at relieving migraine pain and symptoms. Some triptans are accessible as nasal sprays, injections, and tablets. Triptans have side effects such as nausea, dizziness, drowsiness, and muscle weakness. They are not suggested for persons who are at risk of having a heart attack or stroke. Migraine sufferers frequently take beta blockers or antidepressants to avoid headaches and triptans, such as Imitrex or Relpax, once symptoms appear. Although over-the-counter painkillers like aspirin and ibuprofen can relieve many types of headache discomfort, they are less successful with softening migraines. Prescription medicines are also ineffective for many migraine sufferers, and the majority of them can produce harmful adverse effects. For certain migraine sufferers, home treatments may be the best alternative.
Dangers of Over Using Medication
Chronic daily headache:
There is a syndrome known as "medication overuse headache," which is associated with excessive usage of pain relievers such as paracetamol. Excessive use of pain relievers by patients may result in daily headache, also known as chronic daily headache [38], which suggests headache on at least fifteen days in any given month, indicating that the headache is frequent. Several combination medications containing codeine or caffeine may be producing medication overuse headaches. As a result, using these drugs more than three days a week exacerbates the headaches, making it critical to avoid overuse of medication. In such instances, seeking medical advice is important.
Simple Mechanical Techniques to Relieve the Pain of Migraine Attacks
Temperature – both hot and cold:
Apply an icepack or hot water bottle to the hurting area. Some people benefit from taking hot or cold showers, or immersing their hands and feet in hot or cold water. Anyone can utilise this no-risk headache remedy, even pregnant ladies. To relieve neck tightness, apply heat to the back of the neck; for a pulsing headache, ice the temples.
Pressure:
To relieve a headache, press on the pulse points on the side of the forehead or neck. Massage and reflexology: To achieve the best results, a skilled practitioner is required due to the complexity of these approaches. Because osteopathy and chiropractic are likewise stage-managed treatments for preventing injury, they should be practised under the supervision of a trained practitioner.
Biofeedback:
Biofeedback [39] has been used to lessen migraine attacks and suffering. This approach teaches how to manage specific body functions, channel blood to the hands, lower blood flow in the head, and relieve headache discomfort. Once the patient understands the procedure, it can be practised elsewhere. The primary goal is to teach people how to control their physical responses, so relaxing tight muscles and preventing headache discomfort.
Botox:
Botox [40] is a commercial name for botulinum toxin A, a toxin produced by the bacterium that causes botulism. When injected into muscle, the toxin remains in the injected location rather than entering the bloodstream, causing the muscle to relax.
Acupuncture:
Acupuncture involves inserting small needles under the skin to re-support the passage of qi. Acupuncture may help avoid acute migraines and minimise medication treatments with fewer harmful side effects.
Massage:
Rub the temples for temporary relief, or have a massage for your neck, back, head, or shoulders. Having six weekly massage treatments may result in fewer migraines and improved sleep during the massage weeks.
Stretching:
Headache-relieving exercises help address muscle tightness that causes pain. They can be used during a workout or when you have a headache. Try these three exercises: neck range of motion (chin forward, upward, and toward each shoulder); shoulder shrugs (shrug up, up and forward, and up and back); and neck isometrics (press palm into forehead and hold; press hand on each side of the head). Stretch twice a day for 20 minutes every session. Hold the stretch for five seconds, then relax for five seconds. Repeat the stretch three to five times.
Aerobics:
The National Pain Foundation suggested that frequent cardiovascular exercises like brisk walking, riding, or gentle jogging can help reduce migraine intensity and frequency.
Meditation and Yoga:
The National Pain Foundation called for frequent cardiovascular exercise, such as brisk walking, riding, or gentle jogging, to reduce migraine intensity and frequency.
Relaxation exercises:
Deep breathing and listening to music can help people slow down their migraine headaches while also relaxing their minds and bodies.
Transcranial magnetic stimulation:
Deep breathing and listening to music can help people reduce their migraine headaches while also calming their minds and bodies.
Electrode implants:
People with chronic headaches may one day rely on electrodes placed in their necks or brains to give pain relief. This treatment involves surgically implanting an electrode at the base of the skull, near the occipital nerve. In addition, a power source is implanted (near the collar bone or elsewhere in the body) to transmit electrical impulses to the electrode via wire.
Diet and Migraine: [41-44]
There is no migraine-specific diet that alleviates symptoms. Understanding the specific triggers of migraines and avoiding certain dietary triggers may help some sufferers reduce the frequency of attacks. Certain meals, however, can cause migraines in those who are vulnerable. These dishes include:
Devices and surgery: [45,46]


Om Dixit*, Madhuri Pandole, Mishri Fenil Patel, Pandya Khushi Chetan Kumar, Understanding the Migraine from Newer Perspective, Int. J. Med. Pharm. Sci., 2026, 2 (4), 74-83. https://doi.org/10.5281/zenodo.19474360
 10.5281/zenodo.19474360
10.5281/zenodo.19474360
