Oriental University, Indore MP
Asthma attack repeats many times in a day, so it is inconvenient for patient to take medicines repeatedly in an interval. Mostly asthma attack occurs at mid night so, it is very difficult to take medication at mid night for patients. In conventional dosage form, due to first pass metabolism maximum part of drug metabolized. In order to avoid this problem pulsatile form of immediate and burst release of a drug provides drug release at the time of attack and at a particular site. With the help of pulsatile delivery system drug releases with a lag time of 5-6 hours and a burst release of drug at the time of asthmatic attack hence, mid night dosing may be avoided. In the present research work non pareil seed will be used for drug loading and their drug loaded pellets will be coated with enteric coated polymers to delay drug release or to provide lag time. Hence, drug will be released as a burst form at the time of asthmatic attack following lag time i.e during early morning hours. With the use of non pareil seed the delivery of drug at the target site may be achieved by avoiding dose dumping. This may reduce pill burden and mid night time dosing.
Asthma is characterized by chronic airway inflammation, airway hyper-responsiveness, and irreversible airway remodelling, but its pathogenesis is unclear. Mainly asthma treatments rely on long-term inhaled corticosteroids (ICS). Asthma is common chronic disease that affects persons of all ages. People with asthma report impact on the physical, psychological and social domains of quality of life. 1 Asthma is a chronic inflammatory disease of the airways, characterized by hyper responsiveness to a variety of stimuli. The role of circadian rhythms in the pathogenesis and treatment strategies of asthma indicates that airway resistance increases progressively at night in asthmatic patients. In normal lung function, circadian changes are seen, which reaches a low point in the early morning hours. The worsening of asthma at night, is commonly referred to as nocturnal asthma (NA). The dose is administered at bedtime but should release drug during morning hours. The lungs provide an interface between air that we breath in and the bloodstream. When a person breathes, air is drawn in through the nose and mouth and down through the trachea. The trachea divides into two bronchi, a right main bronchus and left main bronchus, to supply each lung. The bronchi divide into smaller bronchi, and then into bronchioles which ultimately terminate in the alveoli – the folded membranes where gas exchange takes place. The bronchi and bronchioles have a muscular layer in the wall which allows them to contract. In an acute asthma attack, this muscular layer contracts and leads to narrowing of the airways. Inflammation may still be present between asthma attacks. This make the airways sensitive and more likely to react asthma triggers and cause an acute asthma attack.2,3
MATERIALS AND METHOD:
Experimental Work
Melting point determination
Melting point of drug sample was determined by using melting point apparatus. The drug sample was taken and placed in a thin walled capillary tube, the tube was approximately 10-12 cm in length with 1 mm in diameter and closed at one end. The capillary was placed in melting point apparatus and heated and when drug sample was melted the melting point of sample powder was recorded.4
Determination of λmax
50 mg of Terbutaline sulphate was weighed and dissolved into 50ml of distilled water, Phosphate buffer pH 6.8 and 0.1 N HCl to prepare a 1000µg/ml stock solution from which a10µg/ml dilution was prepared. Baseline correction was performed using distilled water, Phosphate buffer pH 6.8 and 0.1 N HCl and sample was run between 200-400nm wavelength range in spectrum mode5.
Preparation of 0.1N Hydrochloric acid
0.1N HCl was prepared by diluting 8.5 ml of concentrated Hydrochloric acid to 1000 ml with distilled water.
Preparation of Phosphate Buffer pH6.8
g of monobasic potassium phosphate was weighed and dissolved in 1000 ml of distilled Water to get stock solution of potassium phosphate. 8g sodium hydroxide was weighed and dissolved in 1000 ml of distilled water to get 0.2M sodium hydroxide solution. 250 ml of the monobasic potassium phosphate solution and 22.4 ml of sodium hydroxide solution were mixed and made upto1000ml with distilled water6.
Calibration curve of Terbutaline sulphate
A stock solution was prepared by adding 50mg of drug in 50 ml of water, 0.1N hydrochloric acid and phosphate buffer pH 6.8 separately. The above solution was serially diluted with respective solutions in the concentration in the range of 2- 12µg/ml. The absorbance of the samples was measured at 275nm.
Determination of solubility of Terbutaline sulphate in various medium
The solubility of Terbutaline sulphate in various medium was determined by shake flask method. In this method 5ml of each solvent was taken into a vial and excess amount of Terbutaline sulphate was added. The vials were sealed properly and stirred for 15 min. They were then kept at 37ºC for 24h. After solubilisation of Terbutaline sulphate, an extra amount of Terbutaline sulphate was added to the vials. The process was repeated until saturation solubility of Terbutaline sulphate, indicated by presence of undisclosed drug. The drug solvent mixture was kept at room temperaturefor24hwith continuous shaking. The solution was then filtered and drug content was analyzed spectrophotometrically at 275nm using UV-visible spectrophotometer (Shimadzu-1800).7
Drug–excipient compatibility study
The compatibility of the drug was assessed by drug-excipient interaction study. The drug was mixed with various excipients in a 1:1 ratio in glass vials which were properly sealed and kept undisturbed at25ºC temperature for15days.Afte r30day since compatibility was confirmed by TLC.8
Evaluations
Drug content:
Initially drug loaded pellet (1 pellet) were dissolved in 20 ml phosphate buffer by keeping the flask on shaker for 2 hours whereas time duration for final coated pellets (1 pellet) was 5-6hours in 20 ml phosphate buffer and immediate coated pellet (1 pellet) dissolved in 20 ml HCl for 2 hours. The sample was filtered and estimated by UV spectrophotometrically at 278nm and 273nm.9,10
In-vitro drug release study
The in vitro release was performed according to the USP dissolution apparatus 1basketapparatus at 100 rpm and temperature was taken between 37±0.5°C maintained throughout experiment, the volume of dissolution media was 900 ml in 1000 ml beaker. 0.1 N HCl (pH1.2) was used as dissolution media for first two hours in which initial dose, fourth layer, releases. At the end of second hour dissolution fluid replaced by phosphate buffer of pH 6.8and the apparatus was further operated for five hours. 5 ml aliquots were withdrawn after every 30 minutes interval and replaced with equal amount of fresh dissolution. Samples were filtered an estimated by Spectrophotometer at 278nm.11
Disintegration test
The disintegration tests determine whether capsules disintegrated with in a prescribed time when placed in a liquid medium under the prescribed integral condition. One capsule was placed in each of six tubes of assembly and assembly was suspended in 0. 1NHCl.Discs were added to each tube, temperature was maintained at 37±2°C and disintegration time was noted.12
Stability studies
The stability studies were carried out for a period of 1 month in the stability chamber. The capsule were stored under the condition as prescribed by ICH guidelines (40ºC±2% RH and75±5% RH Q1C). The capsules were withdrawn periodically with an interval of 30 days and analyzed for Disintegration, InVitro drug release, Drug content etc.13,14
RESULT AND DISCUSSION
Preformulation
Melting point Determination: The melting point of Terbutaline sulphate was found to be 118- 120ºC which is same as reported in literature.
Determination of wavelength using UV spectrophotometric analysis: The maximum wavelength of Terbutaline sulphate was found to be 275nm. The reported wavelength is 276- 280nm.
Fig: 1 UV spectrum of Terbutaline in water
Preparation of calibration curves:
The calibration curves of Terbutaline sulphate in various solvent e.g. Distilled water, Phosphate buffer pH6.8 and 0.1NHCl was prepared.
Table No..1: Absorbance data of Terbutaline sulphate in distilled water at 275nm
|
S.No |
Concentration(µg/ml) |
Absorbance |
|
1. |
0 |
0 |
|
2. |
2 |
0.014± 0.001 |
|
3. |
4 |
0.021± 0.001 |
|
4. |
6 |
0.030± 0.001 |
|
5. |
8 |
0.037± 0.001 |
|
6. |
10 |
0.045± 0.001 |
|
7. |
12 |
0.055± 0.0008 |
Fig 2: Calibration curve of Terbutaline sulphate in distilled wate
Table No. .2: Absorbance data of Terbutaline sulphate in phosphate buffer pH 6.8 at 278 nm
|
S.No. |
Concentration(µg/ml) |
Absorbance |
|
1. |
0 |
0 |
|
2. |
2 |
0.035± 0.0008 |
|
3. |
4 |
0.052± 0.0008 |
|
4. |
6 |
0.074± 0.001 |
|
5. |
8 |
0.097± 0.001 |
|
6. |
10 |
0.116± 0.0008 |
|
7. |
12 |
0.133± 0.001 |
Fig. 3: Calibration curve of Terbutaline sulphate in Phosphate buffer pH 6.8 at 278nm
Table No.3: Absorbance data of Terbutaline sulphate in 0.1NHCl at273nm
|
S.No. |
Concentration(µg/ml) |
Absorbance |
|
1. |
2 |
0.013± 0.0008 |
|
2. |
4 |
0.019± 0.0008 |
|
3. |
6 |
0.024±0.001 |
|
4. |
8 |
0.029±0.0008 |
|
5. |
10 |
0.035±0.001 |
|
6. |
12 |
0.041±0.001 |
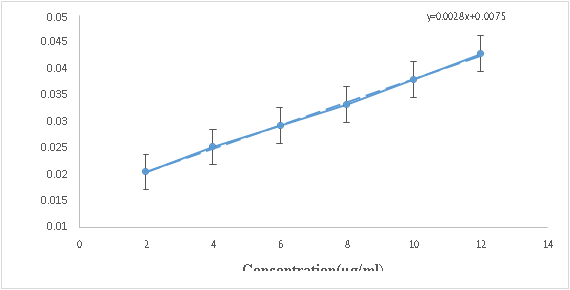
Fig .4: Calibration curve of Terbutaline sulphate in 0.1NHCl at 273 nm
Determination of solubility of Terbutaline sulphate in various medium
The solubility of Terbutaline sulphate in various medium were studied and results of study shown in table7.4:
Table No..4: Solubility data of Terbutaline sulphate indifferent medium at 37°C
|
S.no. |
Solvent |
Solubility |
|
1. |
Distilled water |
210.97mg/ml |
|
2. |
Phosphate buffer pH6.8 |
51.80mg/ml |
|
3. |
0.1NHCl |
63.03mg/ml |
Drug-excipient interaction study
The drug Terbutaline sulphate was found to be compatible with various excipients which were selected for formulation of pulsatile drug delivery. The compatibility was assessed by TLC and retention factors of all ratio found similar. The Rf factor of Terbutaline is 0.34 and mobile phase is Chloroform: Methanol (4:1) and runtime is 30min.
Table No. .5: Drug excipient compatibility study
|
S. No. |
Compound |
Rfvalueat |
||
|
0day |
15days |
3
Att E. Ameen*, Dr. Deepika Gupta, Dr. Sudha Vengurlekar, Dr. Sachin Kumar Jain, Formulation and Evaluation of Pulsatile Drug Delivery System of Bronchodilator, Int. J. Med. Pharm. Sci., 2026, 2 (2), 34-42. https://doi.org/10.5281/zenodo.18495823 | ||

 Att E. Ameen*
Att E. Ameen*
 Dr. Deepika Gupta
Dr. Deepika Gupta
 10.5281/zenodo.18495823
10.5281/zenodo.18495823