Krishna Foundations Jaywant institute of Pharmacy, Wathar, Tal- Karad Dist- Satara 415108 Maharashtra, India
A common dermatological condition that mostly affects the neck, axillae, and groin, acanthosis nigricans (AN) is characterised by velvety, thickened, and hyperpigmented skin.It is frequently linked to endocrine problems, obesity, and insulin resistance. While addressing the underlying systemic causes is essential, topical therapies play a crucial role in improving skin appearance and texture. Phytochemicals—such as natural keratolytics, antioxidants, anti-inflammatory agents, and tyrosinase inhibitors—have gained attention for their efficacy and safety in managing acanthosis nigricans. Compounds like alpha hydroxy acids (lactic and glycolic acid), salicylic acid, urea, vitamin D analogues, and natural antioxidants help promote epidermal turnover, reduce hyperkeratosis, inhibit melanin synthesis, and alleviate oxidative stress and inflammation. Clinical evidence supports the effectiveness of tretinoin and urea in improving pigmentation and texture, while procedures like trichloroacetic acid peels benefit resistant cases. Formulation strategies combining multiple bioactives in creams or chemical peels further enhance therapeutic outcomes and tolerability. Incorporating antioxidants and anti-inflammatory agents provides additional relief by targeting oxidative and inflammatory pathways. Overall, phytochemical-based topical treatments represent a safe, effective, and cosmetically acceptable approach for managing acanthosis nigricans alongside systemic interventions, warranting further research to optimize formulations and confirm long-term efficacy.
The characteristics of Acanthosis Nigricans include dark, rough, hyperkeratotic, and hyperpigmented Plaques or patches dispersed throughout intertriginous areas.1The most frequent cause of Acanthosis nigricans (AN) is hyperinsulinemia and as a paraneoplastic syndrome, which is less common. Additionally, it is a characteristic of various genetic illnesses. Tyrosine kinase growth factor receptor involvement is suggested by indirect evidence in the pathophysiology of AN, signaling 2.It has been shown that acanthosis nigricans is linked to insulin resistance. A metabolic condition known as insulin resistance occurs when target cells are unable to react to normal levels of circulating insulin3.The likely mechanism underlying AN in insulin resistance involves high insulin levels triggering insulin-like growth factor 1 (IGF-1) receptors, either directly or indirectly 2.This causes both to proliferate cell types, as well as papillomatosis and plaques that are clinically noticeable. Acanthosis nigricans is a prevalent skin condition that may indicate a systemic illness that is linked with internal cancer, obesity, diabetes mellitus, and insulin resistance, drug reactions and endocrine disorders4. Acanthosis nigricans is a lesion affects specific skin regions in people who are obese and/or have high blood sugar levels (hyperinsulinemia). Getting rougher corresponds to histological papilomatosis, and the reason for the apparent darkening of the skin is to excessive keratinization. The biochemical processes that lead to the development of this hyperplastic lesion are unknown, but probably involves local growth factors in the skin5. AN can happen anywhere on the body, but typically impacts the groin, the nape, the sides of the neck, and the axillae, the umbilical region, as well as the antecubital and popliteal surfaces. On the vulva, lips, and eyelids, There may be noticeable extensive papillomatosis6. Acanthosis nigricans is a skin lesion that was once thought to be a rare condition linked to severe insulin resistance or visceral cancer. It can be brought on by acquired conditions where antibodies block or accelerate the turnover of insulin receptors, or it can be caused by genetic defects in the action of insulin5. Acanthosis nigricans is a skin disease with multiple aetiologies , exemplified by rough, dark, symmetric, velvety, and thickened emerging plaques ,typically found in the neck, axillae, antecubital popliteal fossae, Inframammary and groin areas7.Numerous endocrine abnormalities are linked to acanthosis nigricans, such as diabetes mellitus, polycystic ovary disease, Cushing syndrome, Addison's disease, hypo- and hyperthyroidism8. AN is strongly linked with all the aspects of the insulin Resistance syndrome, particularly obesity.AN is a key early indicator of obesity syndrome in pigmented populations. People who are particularly susceptible to obesity syndrome, hypertension, dyslipidemia and IR with type II DM can be identified with the help of AN 9.The prime focus of AN treatment are elimination of the underlying medical conditions that result in the velvety, darkened, keratinized patches appeared on the skin4.Managing obesity plays a key role in reversing the entire process, mainly by reducing insulin resistance and the resulting high insulin levels10.
Pathophysiology of Acanthosis Nigricans
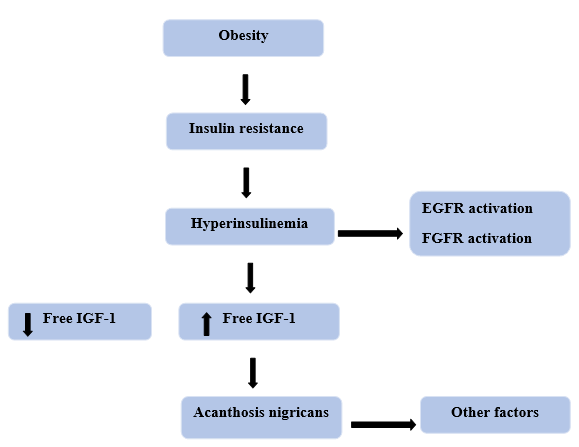
Fig. No 1: Pathophysiology of Acanthosis Nigricans
Factors that promote the proliferation of dermal fibroblasts and epidermal keratinocytes are the cause of acanthosis nigricans. In situations with benign AN, insulin or an IGF has been suggested as a stimulator of increased epidermal cell proliferation. Tyrosine kinase receptors notably the epidermal growth factor receptor and fibroblast growth factor (FGF) seem to be additional mediators involved11.Because of its strong affinity for IGF-1 receptors, insulin may exert strong proliferative effects at high dosages. Additionally, free IGF-1 levels may be higher in obese individuals with high insulin levels, which could accelerate cell growth and differentiation12.There are known syndromic and familial types of AN.Hyperinsulinemia obesity, and craniosynostosis are among the characteristics that many syndromes have in common. They have been further categorized as insulin resistance syndromes as well as FGF defects13. IGF-1 receptors on fibroblasts and keratinocytes are activated both directly and indirectly by elevated insulin levels, which promotes proliferation. The tyrosine kinase receptors FGFR and EGFR are examples of other mediators that might be involved. (insulin-like growth factor, binding protein, insulin-like growth factor 1 receptor, epidermal growth factor receptor, and fibroblast growth factor receptor). AN is typically linked with insulin-resistant disorders, such as obesity, type 2 DM, and polycystic ovary syndrome14.Number of studies indicate that insulin-dependent activation of IGF-1 receptor can encourage the growth of cell and contribute to the development of AN.First, fibroblasts and keratinocytes in culture have IGF receptors. Second, insulin promotes fibroblast growth and replication at high concentrations by bridging the dermo epidermal junction. Lastly, there is a positive correlation between fasting insulin levels and the severity of AN in obese people. Thus, insulin may promote AN by directly activating the IGF-1 signaling pathway12. By raising the amount of free IGF-1 in the blood, hyperinsulinemia may also indirectly aid in the development of AN. IGF binding proteins control IGF-1 activity by extending IGF-1 half-life, delivering IGFs to target tissues, and controlling the amounts of metabolically active "free" IGF-1. In obese individuals with elevated insulin levels, plasma concentrations of free IGF-1 rise as a result of reduced levels of insulin-like growth factor 1 binding protein and IGFBP-2 15.Dermal fibroblasts and the stratum granulosum both express insulin-like growth factor 1, but epidermal basal keratinocytes do not. Theoretically, a systemic decrease in IGFBP-1 and IGFBP-2 brought on by insulin may increase local levels of free IGF-1, which would promote papillomatosis and hyperkeratosis12.
Phytochemicals used in treatment of AN
Keratolytic agents are common terms for substances used to treat hyperkeratosis. The clinical degree of hyperkeratosis is considerably reduced by these substances16. The most common cause of skin darkening is hyperkeratosis1. Hyperkeratosis may also result from increased keratinocyte production. The term keratolytic refers to keratolysis, but the substances do not always cause keratin lysis when used on the skin. This group includes substances such as alpha-hydroxy acids& polyhydroxy acids (AHA& PHA), urea, salicylic acid, resorcinol, retinoic acid, and sulfur17.Keratolytic agents function by inducing desquamation, which is the softening, swelling, and shedding of the cornified epithelium, or outer skin layer18.
For millennia, AHAs have been utilised as exfoliants. These acids include lactic acid (found in milk), glycollic acid (found in sugarcane), malic acid (found in apples), citric acid (found in citrus fruits) and tartaric acid (found in grapes)19.AHAs, particularly lactic and glycollic acid, are employed in peeling chemical solutions to scrape thicker skin in hyperkeratotic disorders and other conditions with excessive keratin accumulation20.Topical application of alpha hydroxy acids in lower concentrations reduces corneocyte adhesion in the lower stratum corneum, thereby thinning thickened skin layers21.Alpha hydroxy acids (AHAs) absorb into the epidermis, accelerating the shedding process of the outermost skin layer while maintaining the skin's natural barrier function22. By increasing hydration, reducing surface charge, and modulating enzyme activity, AHAs weaken the bonds between corneocytes, disrupting desmosomes and ultimately facilitating the shedding of dead skin cells, which in turn stimulates cell renewal23.
SA is also referred as orthohydrobenzoic acid or 2-hydroxybenzoic acid. Wintergreen leaves, sweet birch, and willow bark are sources of salicylates and SA24. SA is the most widely utilized &extensively researched of the currently known keratolytic compounds. SA is thought to decrease intercellular cohesion between corneocytes by dissolving the intercellular cement material and lowering the pH of the stratum corneum, resulting in increased hydration and softening20. SA is a keratolytic agent that reduces hyperkeratosis caused by acanthosis nigricans. In Europe, a formulation for treating AN lesions combines a low dose of 5-luorouracil (0.5%) with SA (10%). A randomized, double-blind Phase 3 study of 166 patients demonstrated the safety and efficacy of combining 0.5% 5-fluorouracil along with 10% SA for treating field cancerization on the face, scalp, and forehead in individuals with multiple actinic keratosis lesions10.10% SA and 10% urea creams effectively reduce hyperpigmentation in AN, with similar efficacy and safety profiles25.Indian patients between the ages of 18 and 50 who had Fitzpatrick skin types 4 or 5 and benign hereditary AN impacting the underarms, regardless of the affection of other usual areas, participated in a retrospective pilot study. Information was obtained from seventeen patients who had axillary AN. For a total of six treatments, patients received a combination salicylic and mandelic acid peel at intervals of two weeks. After the chemical peeling sessions were finished, maintenance was achieved by using a cream comprising cetylated fat esters, urea, and glycollic acid at night for nine months. For a total of nine months, lesions were assessed every three months for improvements in skin thickness and pigmentation. All patients (100%) improved significantly in terms of pigmentation and lesion thickness. In terms of skin thickening improvement, 41% of patients saw very good progress, while 29% experienced moderate progress. 35% showed very good or moderate improvement in pigmentation. The most frequent adverse reactions were temporary redness (100%) and stinging sensation (90%), resolving within 1-2 days. A 9-month follow-up period revealed no recurrence26.
As a crucial element of the skin's natural moisturizing factor, urea significantly contributes to maintaining hydration and structural integrity of the skin27.It is well known that urea has anti-pruritic, hydrating, hygroscopic, penetration-enhancing, keratolytic, proteolytic, and epidermis-thinning properties22. In cases of pathologically dry skin, the diminished ability to retain moisture leads to excessive transepidermal water loss (TEWL). This imbalance triggers increased epidermal cell turnover and disrupts normal shedding processes, ultimately resulting in thickened (hyperkeratotic) and often itchy skin. Common underlying causes link these dermatoses to abnormal expression of genes that encode epidermal structural and catalytic proteins. Urea-based formulations have been utilized for over 100 years, with their effects varying by concentration, to help hydrate the skin, reduce thickening, and enhance the absorption of topical treatments28. The 20% concentration of urea cream is more efficient than the 10% concentration in treating teenage AN-related neck hyperpigmentation29.
AN is a dermatological disorder that typically affects body folds like the axillae and is characterised by hyperpigmentation and skin thickness. There are few known options for treating axillary hyperpigmentation. This study evaluated the efficacy of 0.025% tretinoin cream in the treatment of AN-related underarm darkening. In a split-side research, participants applied 0.025% tretinoin cream to one underarm and a control cream to another for eight weeks, followed by a four-week monitoring period. Efficacy was assessed using narrowband reflectance spectrophotometry and the melanin (M) index. Overall success was assessed using investigator- and participant-global evaluation (IGE and PGE) scales, with side effects monitored. The study was finished by twenty participants. When compared with the control treatment, 0.025% tretinoin cream significantly reduced underarm hyperpigmentation (p < 0.001). After eight weeks, the melanin index decreased by 28.05% ± 12.20% with tretinoin compared to 6.55% ± 12.66% with the control. However, after stopping treatment, hyperpigmentation partially recovered. Compared to 35% with the cream group, 75% of those in the tretinoin group had boosted their IGE by more than 75% by week eight. In a similar vein, just 15% of the cream-based group claimed a PGE enhancement of more than 50%, whereas 75% of the tretinoin group recorded an improvement of more than 75%. The adverse effects were minor, including erythema, peeling, and itching. AN patients axillary hyperpigmentation was significantly improved by 0.025% tretinoin cream, indicating a effective and safe treatment option with not much adverse effects30.
TCA is a superficial chemical exfoliator that destroys the epidermis before repairing and rejuvenating it. TCA (15%) coagulates skin proteins, producing a frosting effect due to its caustic nature. Epidermal necrosis and destruction brought on by protein precipitation are followed by inflammation and the initiation of wound healing processes. The replacement of smoother skin and re-epithelialization result from this.TCA's stability ensures predictable results, with frost intensity indicating peel depth and systemic absorption, making it easier to determine the endpoint. TCA is affordable, easily accessible, safe, and easy to make. Compared to alternative topical options, TCA 15% is a dependable and efficient therapy option for AN. Tretinoin cream requires prolonged use (two months) with frequent applications, and while it improves thickening, it has limited effect on skin darkening. Topical urea, podophyllin, calcipotriol, and salicylic acid, must be applied on a regular basis, whereas a TCA peel requires only 2 to 3 sessions. In addition to being expensive, alexandrite laser and dermabrasion treatments can cause postinflammatory hyperpigmentation. Six female patients showed improvement in AN with TCA peeling, according to Zayed et al.30.
Tyrosinase is a crucial enzyme that relies on copper to facilitate melanin production31.Tyrosinase inhibition is a primary strategy for reducing melanin production, with many inhibitors targeting its catalytic function. TIs are found in most cosmetics and skin-lightening products that are sold commercially.Numerous TIs, such as hydroquinone, kojic acid, L-ascorbic acid, tranexamic acid, arbutin, ellagic acid and azelaic acid have been employed as skin-whitening agents through virtual screening, natural products, laboratory synthesis procedures, and structure-driven molecular docking investigations32. As they produce bioactive chemicals with antityrosinase action, natural sources like fungi, plants, and microbes have recently acquired favour. Because these are more bioavailable and less harmful, many researchers prefer to find inhibitors from natural sources, especially for usage in food, medicine, and cosmetics33.These inhibitors were divided into two parts, mushroom and human tyrosinase inhibitors.
Tyrosinase from the mushroom Agaricusbisporus is commonly utilized as an enzymatic in vitro model for developing skin whitening agents that target human tyrosinase. The majority of research has been conducted using mushroom tyrosinase (mTAR), which is commercially available. The compounds were screened using popular whitening agents like arbutin, hydroquinone or kojic acid as a positive control. Consequently, many mushroom tyrosinase inhibitors have been discovered in recent years, both naturally and synthetically.
Human tyrosinase inhibitors are crucial in inhibiting melanin production and are potential therapeutic agents for treating hyperpigmentation disordersIn an attempt to identify new inhibitors of human tyrosinase, Yoshimori et al. investigated the inhibitory effects of thujaplicins on human tyrosinase and mushroom tyrosinase32.
Natural tyrosinase inhibitors
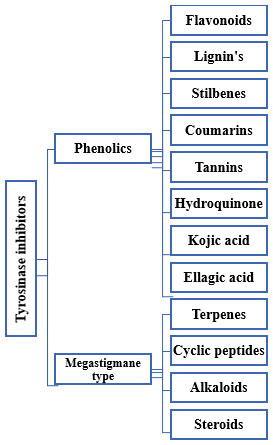
Fig. No 2: Natural tyrosinase inhibitors
Phenolic compounds inhibit tyrosinase by either chelating copper or mimicking the enzyme's natural substrates, thereby reducing melanin production through competitive inhibition34.
Flavonoids show promise as tyrosinase inhibitors by binding to copper ions and forming enzyme complexes. The quantity and positioning of hydroxyl groups on their molecular framework have a significant impact on their efficacy. Higher plants produce secondary metabolites called plant polyphenols, which have a variety of biological functions. Plant seeds, leaves, flowers, and bark contain phenols and pyran rings, which make up flavonoids, one of the most researched polyphenol derivatives35. Researchers have isolated and studied flavonoid compounds from natural sources to find potent tyrosinase inhibitors, assessing their impact on mushroom tyrosinase-Morusyunnanensis, Tibouchinasemidecandra L, mung bean, calamondin peel, Trifoliumnigrescens Subsp. Petrisavi, Bhagwa and Alpiniaofficinarum, Maackiafaurie, Pleurotusostreatus, Potentillabifurca, Arakta cultivar, roots of Garcinia subelliptica, Moruslhou, Pulsatillacernua, Myrsineafricana, Artocapusaltilis, Salvia miltiorrhiza- Carthamustinctorius herbal pair and other various theraputic plants33. Flavonoids make up the largest part of newly found natural TIs. These are classified into six types: flavanols, isoflavones, flavones, flavanones, flavonolsand anthocyanidin. A few flavonoids, such as kaempferol, morin, and quercetin inhibit tyrosinase action, whereas others, like rhamnetin and catechin act as substrates, suppressing tyrosinase action by acting as a cofactor (catechin) or a free radical scavenger35.
The three main building blocks of the lignan family give rise to a diverse array of complex compounds. Tyrosinase inhibitory action has so far been examined in lignans and lignan glycosides extracted from the exocarps of Marrubiumvelutinum, Castaneahenryi, Pinellia ternate, Crataeguspinnatifida and Marrubiumcylleneum. The majority of these substances showed mild suppressive effects on mushroom tyrosinase33.
Red wine and grapes contain resveratrol, a widely recognised stilbene renowned for its ability to inhibit tyrosinase. The tyrosinase inhibitory action of a number of stilbene derivatives, both synthetic and natural, has been investigated. However, investigations using enzymatic assays have demonstrated that resveratrol decreases tyrosinase's oxidation of L-tyrosine at 100 µM but does not affect tyrosinase's diphenolase activity36.
Coumarins are found in many plants, particularly cassia cinnamon and tonka beans, and are known to be effective tyrosinase inhibitors36.Researchers have investigated various coumarin derivatives for their potential as tyrosinase inhibitors. These compounds include 3-aryl and 3-heteroarylcoumarins, umbelliferone, coumarinolignoid, 8’-epi-cleomiscosin, esculetin, hydroxycoumarins, phenyl coumarins, and hybrids like coumarin-resveratrol, among others33.Coumarins inhibit tyrosinase activity by chelating copper ions or forming complexes with the enzyme.
Tannins have been demonstrated as severe inhibitors of tyrosinase, an enzyme involved in melanin production. Valonea tannin, a hydrolysable tannin derived from acorn shells, has a high tyrosinase inhibition. It inhibits tyrosinase using a competitive-uncompetitive mechanism and binds non-selectively via hydrogen bonds and hydrophobic interactions. This tannin also exhibits antioxidant and copper ion chelation properties, which may enhance inhibition37. Condensed hop tannins, which are primarily composed of (epi)catechin and (epi)gallocatechin subunits, also inhibit tyrosinase significantly. These tannins inhibit tyrosinase via competitive-uncompetitive mixed mechanisms, binding to both active and inactive sites on the enzyme38.
1, 4-Hydroquinone is frequently used to treat hyperpigmentation and can be found in wheat, tea, beer, coffee, and berries. Through a variety of processes, including as covalent histone binding, copper contact at the site of action, and acting as an inadequate substrate for tyrosinase, hydroquinone prevents the formation of melanin. Hydroquinone was considered the gold standard for treating hyperpigmentation for a long time35. The leaves of blueberries, pears, bearberries, and cranberries contain beta-arbutin, a beta-D-glucopyranoside of hydroquinone39.In cultured melanocytes, beta-arbutin decreases tyrosinase inhibition in a dose-specific manner40.
Tyrosinase activity is notably suppressed by kojic acid, a well-established inhibitor. Kojic acid effectively reduces the formation of pigmented products and oxygen consumption when tyrosinase oxidizes norepinephrine, DL-DOPA, and dopamine41. Fungal-derived kojic acid is a slow-binding tyrosinase antagonist utilised in food preservation and skin-whitening products. It exhibits mixed inhibition of diphenolase activity and competitively inhibits monophenolase activity by chelating transition metals such as Cu²? and Fe³?35.
Numerous plants contain ellagic acid, a naturally existing polyphenol that can be found both free and as a component of ellagitannin glycosides. Dicotyledonous woody plants belonging to the genera Eucalyptus (Myrtaceae), Castanea (Fagaceae), and Quercus (Fagaceae) contain it. Additionally, it is present in many fruits and vegetables that people frequently eat, including as walnuts, cherries, and grapes. EA has recently been demonstrated to prevent UV-induced skin pigmentation. According to in vitro studies, EA suppresses melanogenesis via inhibiting tyrosinase activity.Tyrosinase molecules chelation of copper atoms is what causes this inhibition42.
Megastigmanes, along with other plant-derived secondary metabolites such as terpenes, alkaloids, cyclic peptides, and steroids, have been identified as potent tyrosinase inhibitors in herbal medicine research. These compounds inhibit melanin biosynthesis and are thought to be beneficial in the treatment of hyperpigmentation-related skin conditions like acanthosis nigricans. Megastigmanes are C13-norisoprenoid compounds found in plants such as Panax ginseng, Camellia sinensis, and Cucumissativus. They possess antioxidant and enzyme inhibitory properties, including tyrosinase inhibition. According to Zaidi et al. (2019), megastigmane glycosides and derivatives inhibit tyrosinase activity, preventing melanin overproduction that causes darkened skin patches in hyperpigmentary disorders43.
Terpenes that show competitive inhibition against tyrosinase include triterpenes in Glycyrrhiza glabra and monoterpenes in Melaleuca alternifolia43.
Cyclic peptides, such as those found in Moringa oleifera, have radical-scavenging activity and mild tyrosinase inhibition properties, which contribute to depigmentation44.
Alkaloids (like berberine and piperine) that suppress melanogenesis via tyrosinase modulation and are common in herbal formulations targeting metabolic-related hyperpigmentation including acanthosis nigricans43,45.
Steroids (phytosteroids like diosgenin from Dioscoreavillosa) that regulate melanocyte function and inflammatory responses, complementing depigmenting treatments in Ayurvedic or Chinese herbal regimens45.
Oxidative stress plays a crucial role in various bodily biochemical reactions, including melanin production46.Excessive production of reactive oxygen and nitrogen species can lead to various diseases. Neutralizing these oxidants may help alleviate oxidative stress. Antioxidant phytochemicals, which are found in many foods and medicinal plants, are crucial for both avoiding and treating oxidative stress-related chronic diseases47. Antioxidant-rich phytochemicals are abundant in various foods, including fruits, grains, vegetables, and certain plants.Many common fruits, such as grapes, berries, guava, and pomegranates are particularly high in these beneficial compounds. Additionally, certain wild fruits, including those from Eucalyptus, Melastoma, Eurya, and Lagerstroemia species, exhibit high antioxidant activity and phenolic content. Antioxidant substances like catechin, kaempferol, and gallic acid are also abundant in fruit waste, including peels and seeds. Certain vegetables, like lotus root Chinese toon bud, and broccoli, soy bean (green), sweet potato leaf, exhibit high antioxidant activity and phenolic content. Pigmented rice, such as red, black, and purple rice, has a high concentration of antioxidant phytochemicals (tannins and flavones) among cereal grains47. Another topical treatment for AN is calcipotriene, a vitamin D analog. By raising cyclic GMP levels and keratinocyte intracellular calcium, it is believed to suppress keratinocyte proliferation and encourage differentiation4. Antioxidants counteract reactive oxygen species, shielding cells and tissues from damage. The skin's antioxidant defense system comprises both enzymes and non-enzymatic compounds. Some enzymatic antioxidants like vitamin C, vitamin E, lipoic acids, and resveratrol. These molecules remove free radicals, neutralize singlet oxygen in the cell membrane, prevent lipid peroxidation, inhibit oxidative and mutagenic activity on lipoic acids on DNA, and repair endogenous antioxidant systems48.
The body's reaction to damaging stimuli, including infections or environmental elements, is inflammation, which aims to reduce damage to tissues and encourage healing. Sustained inflammation and a chronic pro-inflammatory state can result from prolonged activation of detrimental signalling pathways and excessive release of inflammatory mediators. A low-grade inflammatory state has been associated with a number of degenerative conditions and long-term health problems, including diabetes, obesity, cancer, cardiovascular disease, and arthritis. Many inflammatory disorders are treated with both non-steroidal and anti-inflammatory steroidal medicines. Alkaloid colchicine, triterpenoid saponin escin, methoxy phenol capsaicin, lignan bicyclol, monoterpene borneol, and flavonoid quercetin are typical examples. These plant compounds can alleviate disease by modulating molecular pathways, either by boosting anti-inflammatory signals or suppressing pro-inflammatory ones.49.
Curcumin –
Curcumin has anti-inflammatory activity. Research demonstrates curcumin’s benefits in controlling skin inflammation, enhancing skin healing, and decreasing epidermal thickness without causing adverse inflammatory changes. Although direct clinical trials in AN are limited, curcumin has shown promise in improving conditions characterized by hyperpigmentation, insulin resistance, and chronic inflammation, which are key factors associated with AN. Its ability to modulate metabolic syndromes adds to its theoretical usefulness in AN management. (
Neem –
Neem, known for its antioxidant and anti-inflammatory activities, can help reduce skin inflammation, improve texture, and support wound healing. The active phytochemicals in neem include nimbin, nimbolide, and quercetin.
Currently used phytochemicals in inflammatory diseases/disorders-
Colchicine, also called as meadow saffron or autumn crocus, is an alkaloid found in the plant Colchicum autumnale L. (Colchicaceae). Colchicine slows leukocyte and other inflammatory cell proliferation, reduces urate crystal inflammation, and inhibits microtubule polymerisation via binding to tubulin50.
Horse chestnuts (Aesculushippocastanum L.) contain escin, a triterpenoid saponin with anti-inflammatory properties. In traditional Chinese medicine, eschin is used to treat cerebral oedema and chronic venous insufficiency. According to recent studies, escin can stop swelling in inflammatory tissues by lowering vascular permeability51.
Various non-steroidal pharmaceuticals and phytochemicals are analgesic and anti-inflammatory. The FDA has approved capsaicin as a topical analgesic for the treatment of neuropathic pain resulting from postherpetic neuralgia. It is available in powder, creams and patch forms, as well as in some dietary supplements48. Capsaicin, the active compound from chili peppers, has well-documented anti-inflammatory, antioxidant, and depigmenting effects that make it relevant in the context of hyperkeratosis and hyperpigmentation for dermatological applications.
4. Bicyclol-
Bicyclol is a synthetic material derived from Schisandra C, a lignin extracted from the Chinese medicinal herb Schisandrachinensis Fructus Baill. The Chinese Medical Association approved these anti-inflammatory drugs for liver issues. Among the modes of action include cytochrome P-450 stimulants, free radical-scavenging HSP70 stimulants, and protein kinase C inhibitors52,53. A synthetic substance called bicyclol, which comes from Schisandra C, has anti-inflammatory qualities that could help with hyperkeratosis or hyperpigmentation45.
Several essential oils include borneol, a bicyclic monoterpene with a strong, bitter taste and scent. Research shows that borneol is effective in lowering inflammatory responses and associated issues54. For instance, borneol is employed to alleviate weariness, worry, and insomnia in Chinese medicine. In addition to providing anaesthesia and relief from pain for burns, wounds, and stomach pain, borneol also cures rheumatism, ulcers, haemorrhoids, and skin conditions. More precisely, it is well recognised to reduce anxiety, digestive problems, stress, inflammation, and pain55.
Pineapple juice and stems include a class of enzymes called bromelain that break down proteins. Inflammatory pathways are triggered by bromelain, resulting in the production of chemicals that reduce pain and inflammation56.When inflammation results in excessive cytokine release, it inhibits the generation of TNF-α, IL-1β, and IL-6 by activated immune cells49.
Curcumin has anti-inflammatory activity. Research demonstrates curcumin’s benefits in controlling skin inflammation, enhancing skin healing, and decreasing epidermal thickness without causing adverse inflammatory changes. Although direct clinical trials in AN are limited, curcumin has shown promise in improving conditions characterized by hyperpigmentation, insulin resistance, and chronic inflammation, which are key factors associated with AN. Its ability to modulate metabolic syndromes adds to its theoretical usefulness in AN management.
Neem, known for its antioxidant and anti-inflammatory activities, can help reduce skin inflammation, improve texture, and support wound healing. The active phytochemicals in neem include nimbin, nimbolide, and quercetin.
Current treatment
Current treatment for AN primarily focuses on treating the root causecause such as insulin resistance, obesity, or malignancy, along with symptomatic management of the skin changes. Topical treatments include keratolytics (e.g., retinoids, lactic acid), vitamin D analogs, and other agents aimed at exfoliating and lightening the thickened, hyperpigmented skin. Cosmetic procedures like laser therapy and chemical peels are sometimes used7.Correcting the underlying disease process should be the main goal of AN treatment. Weight loss in AN associated with obesity may resolve hyperkeratotic lesions, but correcting hyperinsulinemia can reduce the AN lesion burden. While surgical tumour removal is the main treatment for malignancy-related AN, stopping the causative substance frequently leads to resolution in drug-induced AN. While the primary goal of AN therapy is to treat the underlying cause, cosmetic resolution of AN lesions can have a significant effect on patients and their quality of life4.
One of the first-line treatments for AN is thought to be topical retinoids4. Since there is frequently no discernible underlying disease process, these are the only treatments available for UNAN. Retinoids restore normal epidermal thickness, normalize epidermal turnover, and correct hyperkeratosis7.Tretinoin (0.025,0.05%) and adapalene (0.1%) alter epidermal turnover as well as epidermal keratinization ,treatment duration 4-14 weeks57.
A common vitamin D analog used to treat a variety of dermatoses is calcipotriol7.It is believed to promote differentiation by preventing keratinocyte growth and increasing intracellular calcium and cyclic GMP levels in keratinocytes58.By lowering the quantity of active keratinocytes available for target, it might lessen the cutaneous effect of insulin. An obese woman with AN and nipple hyperkeratosis reported that using calcipotriol cream for three months significantly improved the lesions7.
Trichloroacetic acid (TCA), a chemical peeling agent, has been successfully used to treat AN7. Trichloroacetic acid is a chemical exfoliation agent that destroys the epidermis and then repairs and rejuvenates it58.TCA causes skin protein coagulation and precipitation, which results in epidermal necrosis. Smoother skin and re-epithelialization follow this destruction, which is accompanied by swelling and wound healing. TCA has several advantages, including safety, accessibility, low cost, and ease of preparation4. When compared to alternative topical treatments, TCA 15% is a safe and effective therapeutic option for AN58. In randomized controlled trials, TCA chemical peels at 15% concentration were found to be more effective than glycolic acid peels59. TCA peels reduce the thickened, hyperpigmented skin thickness and appearance, improving AN severity scores after several treatment sessions with mostly mild and self-limited side effects. TCA can be considered a stronger procedural option when topical creams alone are insufficient or for adjunctive therapy60. Successful trials of glycolic acid (GA) peels have also been conducted in AN, and concentration ranged from 30% to 70%61.
FixdermaNigrifix cream is a specialized topical formulation designed to treat the hyperpigmentation and thickened skin of acanthosis nigricans. Its key ingredients and their roles are:
Retinol: A vitamin A derivative that acts as a powerful exfoliant by stimulating skin cell turnover, removing coarse, keratinized skin layers, and smoothing the skin. It is considered a first-line treatment for acanthosis nigricans.
Lactic Acid: A mild exfoliant and moisturizing agent that loosens bonds between dead skin cells to reduce pigmentation and skin hardness, while hydrating the skin.
Urea: A keratolytic and humectant that softens rough, thickened skin by breaking down hardened cells and retaining moisture, which helps strengthen the skin barrier.
Tea Tree Oil: An essential oil with anti-inflammatory and soothing properties that helps calm dry and irritated skin, reducing discomfort associated with acanthosis nigricans.
Sweet Almond Oil and Jojoba Oil: Added as premium moisturizing agents to nourish sensitive skin areas prone to acanthosis nigricans such as armpits and groin.
Nigrifix cream works as a gentle exfoliator and deep moisturizer to improve the skin texture, even out pigmentation, and prevent further skin damage. It is non-greasy and suitable for sensitive skin locations. Regular application helps visibly reduce the dark leathery patches typical of acanthosis nigricans
Advantages & limitations- Herbal Vs Synthetic-
Advantages-
Limitations-
Advantages-
Limitations
Table No. 1 Summary table:
|
Aspect |
Herbal Formulations |
Synthetic Formulations |
|
Active ingredients |
Natural phytochemicals, antioxidants, AHAs |
Retinoids (tretinoin), urea, salicylic acid, glycolic acid |
|
Evidence Base |
Limited clinical trials, traditional use |
Strong clinical trial support and safety data |
|
Onset of action |
Slower, gradual improvement |
Faster visible results within weeks |
|
Safety profile |
Generally safer, fewer side effects |
Potential irritation and dryness |
|
Mechanism |
Exfoliation, anti-inflammatory, antioxidant |
Exfoliation, keratolysis, pigment inhibition |
|
Suitability |
Mild to moderate cases, sensitive skin |
Moderate to severe, resistant cases |
|
Accessibility & Cost |
Often cost-effective and accessible |
Prescription-based, higher cost |
CONCLUSION
Phytochemical approaches offer a promising and safer alternative in the topical management of acanthosis nigricans. Plant-derived compounds with keratolytic, antioxidant, anti-inflammatory, and tyrosinase-inhibitory properties can effectively target the major pathogenic mechanisms underlying the condition, including hyperkeratosis, oxidative stress, and melanogenesis. Bioactive agents such as flavonoids, polyphenols, and alkaloids not only improve skin texture and pigmentation but also exhibit fewer adverse effects compared to conventional synthetic treatments. Future research should focus on standardizing formulations, determining optimal concentrations, and conducting clinical trials to validate the long-term safety and efficacy of phytochemical-based topical therapies for acanthosis nigricans.
Consent for Publication
This manuscript does not contain any individual or identifiable participant data; therefore, no specific consent for publication is required.
Conflicts of Interest: Authors Declares that No any Conflict of Interest.
REFERENCES

Madhuri Patil*, Shivani Yevale, Dhanshree Thavare, Vishwajit Shinde, Vedantika Shinde, Phytochemical Approaches in Topical Treatment of Acanthosis Nigricans, Int. J. Med. Pharm. Sci., 2026, 2 (4), 141-155. https://doi.org/10.5281/zenodo.19562679
 10.5281/zenodo.19562679
10.5281/zenodo.19562679
